
Advanced Angioplasty for Complex Heart Blockages in Ahmedabad Apollo CVHF Heart Institute
Not all heart blockages are straightforward. Some are severely calcified, making them too hard for a conventional balloon to open. Others are located at critical branch points in the coronary arteries, while some affect the left main coronary artery, the most important artery supplying the heart. In other cases, patients have chronic total occlusions (CTO), where the artery has been completely blocked for months or even years.
Many patients with these complex coronary artery blockages are told that bypass surgery (CABG) is their only option. However, in many cases, this is not true. With the right expertise, advanced imaging technology, and modern complex coronary angioplasty techniques, these blockages can often be treated successfully with coronary angioplasty, helping patients avoid open-heart surgery.
Dr. Kulin Sheth, an experienced Interventional Cardiologist in Ahmedabad, specialises in advanced angioplasty and complex coronary interventions at Apollo CVHF Heart Institute, Bodakdev, Ahmedabad. He has extensive experience treating challenging heart blockage cases that other operators may decline, using a thoughtful, evidence-based approach to deliver safe and effective heart blockage treatment.
When Is a Blockage Considered 'Complex'?
A blockage is considered complex when it has one or more features that make standard angioplasty technically challenging or risky:
- Heavy calcification: calcium deposits within the artery wall make the vessel rigid and difficult to dilate with a conventional balloon
- Left Main Coronary Artery (LMCA) disease: the left main artery supplies the majority of the heart's blood supply, making blockages in this location particularly high-risk and technically demanding
- Bifurcation lesions: blockages at the point where an artery divides into two branches, requiring specialised techniques to treat both vessels
- Chronic Total Occlusions (CTO) : arteries that have been completely blocked for more than 3 months, requiring advanced wiring techniques to cross the blockage
- Long or diffuse disease: blockages spanning a large portion of the artery
- Previously placed stents that have re-narrowed (in-stent restenosis)
- Post-bypass graft disease: blockages in coronary artery bypass grafts
Advanced Technologies Used
Intracoronary Imaging Seeing Inside the Artery
- IVUS (Intravascular Ultrasound) is a miniature ultrasound probe on a catheter that provides detailed cross-sectional images of the artery from inside. IVUS precisely measures the size of the artery, the extent and distribution of calcium, the degree of stent expansion, and the presence of complications. It guides optimal stent sizing and deployment, significantly improving outcomes.
- OCT (Optical Coherence Tomography) a light-based imaging technology providing even higher-resolution images of the artery wall than IVUS. OCT can identify fine structural details such as plaque characteristics, tissue coverage of previously placed stents, and the precise edges of a blockage. It is the gold standard for assessing stent deployment quality and diagnosing the cause of stent failure.
Using IVUS and OCT rather than relying on X-ray alone allows Dr. Sheth to make more precise treatment decisions leading to better stent placement, fewer complications, and improved long-term outcomes.
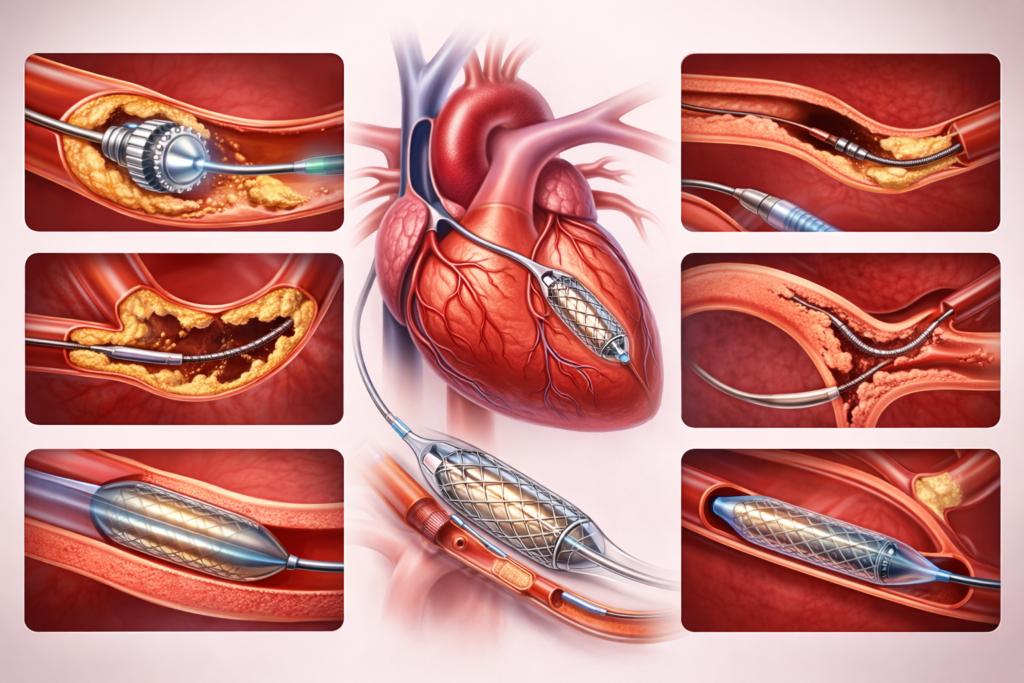
Advanced Treatment Techniques Breaking Through Difficult Blockages
- Rotablation (Rotational Atherectomy): a high-speed rotating burr that drills through severely calcified, rock-hard blockages that cannot be opened with a conventional balloon. The burr pulverises calcium into microscopic particles that are safely absorbed by the body, allowing the artery to be dilated and stented effectively.
- IVL (Intravascular Lithotripsy Shockwave): a newer technology that uses sonic pressure waves similar in principle to kidney stone treatment to fracture calcium deep within the artery wall. IVL is particularly effective for calcification embedded in the wall rather than on the surface, complementing Rotablation in certain situations. It can be used with a standard balloon catheter and requires less technical complexity than Rotablation in some cases.
- CTO (Chronic Total Occlusion) Intervention: opening arteries that have been completely blocked for an extended period. CTO angioplasty is one of the most technically demanding procedures in interventional cardiology, requiring specialised guidewires, microcatheters, and techniques such as retrograde crossing (approaching the blockage from the other direction through collateral vessels). Successful CTO recanalization can restore blood flow to areas of the heart that have been starved of oxygen for months or years.
- LMCA (Left Main Coronary Artery) Intervention: Stenting the left main artery requires precise planning, intracoronary imaging (IVUS or OCT), and meticulous technique. In selected patients, LMCA angioplasty is a safe and effective alternative to bypass surgery, particularly in patients at high surgical risk.
- LMCA (Left Main Coronary Artery) Intervention: stenting the left main artery requires precise planning, intracoronary imaging (IVUS or OCT), and meticulous technique. In selected patients, LMCA angioplasty is a safe and effective alternative to bypass surgery, particularly in patients at high surgical risk.
- Bifurcation Stenting: treating blockages at branch points using specialised two-stent techniques (such as DK Crush or Culotte) when the side branch cannot be protected with a single stent. Bifurcation intervention requires careful planning and precise execution to achieve a good result in both vessels.
A Word About Bypass Surgery
Bypass surgery (CABG) is an excellent and well-established treatment for coronary artery disease, particularly for patients with multi-vessel disease, diabetes, or severely reduced heart function. It is not the wrong choice for many patients, and Dr. Sheth will always be honest when bypass surgery is genuinely the better option for a particular case.
However, many patients are referred for bypass surgery with complex blockages that can, in experienced hands with the right technology, be effectively treated with angioplasty. The decision between angioplasty and bypass surgery should always be made after a full and honest discussion with all the options clearly laid out, and with the patient’s preferences and circumstances fully considered.
If you have been told bypass surgery is your only option, a second opinion from an experienced complex PCI operator is a reasonable and worthwhile step before committing to a major surgical procedure.
Location: Where Are Complex Procedures Performed?

Apollo CVHF Heart Institute
- +91 7096 800 800
- Pakwan Cross Road, Sarkhej - Gandhinagar Hwy, opp. GNFC Tower, next to l.O.C petrol pump, Bodakdev, Ahmedabad, Gujarat 380059
- Angiography, Angioplasty, Pacemakers & Devices (ICD, CRT-D), Structural Heart Procedures (ASD/VSD/PDA Closure, TAVI), Complex Coronary Work (LMCA, Bifurcations, IVL, Rotablation)
- Open 24 hours
Dr. Kulin Sheth's Approach
Dr. Sheth is known for a calm, thorough, and patient-centred consultation style. He takes time to listen, never rushes through an appointment, and explains findings clearly so that patients leave with a genuine understanding of their heart health and what needs to be done, if anything.
Patients also appreciate that Dr. Sheth only recommends investigations that are genuinely needed. There are no unnecessary tests, no unnecessary procedures, and no unnecessary alarm.
Complex Doesn't Always Mean Inoperable
Book a consultation or send your angiography for review. +91 9725551563
Call or WhatsApp: +91 9725551563 | Sheth Heart Clinic, Bopal, Ahmedabad
FAQs
Advanced angioplasty refers to specialized percutaneous coronary interventions (PCI) required for high-risk, technically demanding blockages that standard techniques cannot safely open. Dr. Kulin Sheth performs these complex procedures at advanced cardiac catheterization laboratories in Ahmedabad, utilizing specialized equipment and precision technology to treat severely calcified arteries, multi-vessel disease, and left main coronary artery obstructions.
For severe calcium deposits that prevent standard balloons from expanding, Dr. Kulin Sheth utilizes advanced plaque-modification therapies:
Rotational Atherectomy (Rotablation): A high-speed, diamond-tipped burr that drills through rock-hard calcium to soften the blockage.
Intravascular Lithotripsy (IVL / Shockwave): A cutting-edge balloon catheter that uses acoustic shockwaves to safely fracture calcium within the artery wall, ensuring optimal stent expansion.
Chronic Total Occlusions (CTOs) are old, completely closed blockages (lasting longer than three months) that traditionally required open-heart bypass surgery. Dr. Kulin Sheth utilizes advanced CTO-PCI techniques, including microcatheters, specialized high-penetration guide wires, and retrograde access (approaching the blockage from behind via collateral blood vessels) to safely cross and open 100% blockages without surgery.
Complex blockages carry a higher risk of complications if stents are incorrectly sized or under-expanded. Dr. Kulin Sheth utilizes Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT) to look inside the blood vessel in real-time. This advanced imaging allows for precise measurement of calcium depth, accurate stent selection, and absolute confirmation that the stent is perfectly deployed against the artery wall.
Yes. Many patients with complex or multi-vessel blockages are initially referred for open-heart Coronary Artery Bypass Grafting (CABG). Dr. Kulin Sheth provides specialized second opinions at Sheth Heart Clinic in Ahmedabad to evaluate if the patient is a candidate for high-risk, advanced angioplasty (CHIP-PCI), offering a minimally invasive alternative with faster recovery times for eligible individuals.